
10 Questions to Ask Your Urologist During your Kidney Cancer Appointment
1. What does it mean that I have a kidney cancer mass?
If you have been told that you have kidney cancer than that means that there is a mass on your kidney which has been deemed to have cancer in it. Usually this means that the cancer has started from the kidney. Rarely, there are instances in which there is cancer from somewhere else that has spread to the kidney.
The diagnosis of kidney cancer will typically come from one of two ways. Either you had a biopsy (procedure where the mass was sampled) or after surgery when the mass was either removed or the whole kidney was removed.
As you read this post, I am going to give you all the prepwork that you need to make sure you are seeing a good urologist and that you will understand exactly what he/she is trying to describe to you about your situation. Kidney cancer is pretty straightforward in how we manage it and it really helps to understand why you’re being recommended a particular treatment.
Now for the purpose of this post, I am only going to be talking about kidney cancer that has not spread. Metastatic kidney cancer, or kidney cancer that has spread, is a totally different topic and I’ll try and do a post on that in the future.
2. Are there any signs that the kidney cancer has spread?
This question gets to the bottom of how this should be treated. There are different treatment options if the cancer has spread or is just located within the kidney.
The way that the urologist can tell if it has spread is looking at your x-rays and also making sure that you have had all the tests.
Usually this will entail a CT or MRI of your abdomen (belly) and some sort of imaging of your chest (either a chest x-ray or chest CT scan). Sometimes in more advanced cancers there will be other tests that will have been ordered but typically speaking we just need to image from your neck down to your pelvis. What we are looking for is signs of spread to the lungs, liver, bone, or lymph nodes. Oftentimes, these tests are normal with the exception of the kidney mass.
3. Can I see the images?
The urologist should be able to pull up your films on his/her computer. They should either have access to the films from the hospital and/or you should bring a copy of the disk from wherever you had your imaging done. By looking at the images, you will get a better understanding as to what the mass looks like as well as why the urologist is going to recommend a particular treatment option.
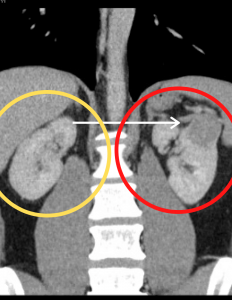
As an example, let’s go over the CT on the left. To orient yourself, just imagine that you are looking at someone in a CT form. So the left side of the image is actually the right side of the body. At the top of the image, we have the bottom of the lung cavity. The two circles show the right and left kidney.
Yellow Circle: This is a CT of the right kidney. It has a normal kidney bean shape and overall is an example of a normal kidney.
Red Circle: The white arrow here shows an example of a solid kidney or renal mass. You can see how it is within the kidney but also has a bulge that is distorting the edge of the kidney. This is a concerning kidney mass for kidney cancer.
So when I look at that image, I will talk about doing a kidney biopsy to see if it has cancer. If the biopsy does show cancer, I can tell that surgically I should be able to remove the mass but not have to remove the whole kidney. This is best seen by looking at the actual x-ray and seeing where and how big the mass is.
So make sure to ask them to show you the films so you can understand the treatment that you are being offered.
4. What is my kidney function?
When a doc is looking at treatment choices, a key point that must be reviewed is how will this affect your overall kidney function. This is important because some treatments may impact your kidney function and increase the likelihood of developing chronic kidney disease.
Having chronic kidney disease (CKD) is not the same as having dialysis but may affect how certain medications will be given, whether new medications need to be prescribed, and potentially affect what diet you should have. Your baseline kidney function is one of the factors that we consider when we debate removing just the kidney cancer mass versus the whole kidney.
5. Wait a sec, you are recommending treatment and don’t even know for sure I have cancer?
So as I mentioned above, there is a measurement called enhancement when we are reviewing your images.
Depending on the size of the kidney cancer bump, if a kidney mass enhances, then there is ~75% chance that the mass is malignant, or cancerous. If there is enough concern, we may say that we gotta head to the operating room for treatment just based on the picture.
In other instances, it is wise to sample the mass first to confirm that there is really cancer there or not. This is called a renal mass biopsy. We would recommend this if the mass is smaller or doesn’t have as many concerning features.
A renal mass biopsy is typically done with the help of the radiologist. He/she will use imaging–either a CT or ultrasound–to verify the location of the mass, numb up the skin, and then poke the mass and remove small slivers of tissue. These slivers will be sent to the pathologist to try and confirm whether the mass has cancer cells or not.
Over the years, the pathologist has gotten better at being able to give these answers for kidney cancer masses. After the biopsy is done, you will usually be able to go home that same day and follow up with the urologist in about a week or so to review the results.
6. Should I have the whole kidney treated or just the mass?
There are several factors that come into play as to whether the treatment recommendation is to remove (or treat) the mass alone or remove the whole kidney.
First and foremost, it is dependent on where and how big the mass is. Oftentimes, a kidney mass is growing on the outer part of the kidney. This makes it technically easier to just remove the mass and leave the rest of the kidney there. Other times the mass is too big, or too close to other important structures, that removing just the mass is too difficult or dangerous. So when you review the images with the urologist, he/she will describe why he/she feels that a partial or a radical nephrectomy is indicated.
Another factor to consider is your overall kidney function. In some instances, the risk of developing kidney failure is very high. In this case, the urologist may take the chance of a riskier surgery to help preserve what kidney function you have and try and prevent the need for dialysis.
7. So, is surgery the only treatment option?
Maybe.
If the mass is too big (i.e. greater than 3 cm) than typically some form of surgery is the best treatment.
However, if the mass is smaller (<3 cm) then there are choices.
One choice is a surgery which is called a partial nephrectomy which is surgical removal of the mass, but not the whole kidney.
Another choice would be an ablation. This is commonly where you are taken to the radiology department. Either an ultrasound or CT will be used to locate the mass. You will be given a local anesthetic (something to numb the side) and medication in the IV. Sometimes the radiologist will need you to have a general anesthetic. Probes (think of them as really long needles) are then placed under x-ray guidance into the mass. The number of probes is dictated by the size of location of the mass.There are usually one of two ablation procedures done for kidney cancer.
There are two kinds of ablation treatments. One is cryoablation and the other is radiofrequency ablation. Again, either is acceptable. They just use temperature and energy in different ways to kill the cancer.
Some of the decision factors in deciding on ablation versus surgery are the size of the mass and the location of the mass. If the mass is bigger than 3 cm, then surgery offers a better success rate.
Additionally, for some tumor locations, an ablation procedure is technically difficult in that it may lead to damage to the kidney drainage tubes (ureter), the intestines, liver, spleen, etc. On the other hand, some patients may not be good candidates to have a major surgery and an ablation provides a slightly simpler treatment route. For these patients, an ablation may be a better option than surgery. So again, it’s really important to understand why the urologist is recommending one treatment over the other.
8. Ok, so they are telling me to have surgery, should this be done laparoscopically (or robotically) or via the traditional (open) approach?
This gets back to why I said (broken record here) before to have the urologist review your images with you. When you are able to see your images, the urologist should be able to explain why he/she thinks that one approach is better than the other.
The advantage of laparoscopy is that there are smaller incisions and a quicker recovery. The disadvantage is that sometimes prior surgical scars and/or scar tissue within the belly may prevent this from being an option. Another factor when making this decision is the size of the mass. If the mass is too big, then laparoscopy isn’t an option.
Lastly, if your kidney function is poor to start sometimes it is safer to remove the mass through an open incision as it may be easier for the doctor to preserve kidney function doing it through this route.
9. Can you go over my pathology report?
After surgery you will typically follow-up in the office in 1-2 weeks so that the doc can see how you are recovering from kidney cancer surgery and review your pathology report.
The pathology report will go over what kind of kidney cancer you have. There are several subtypes and sometimes this will impact your survival.
The report will talk about the surgical margins. If you imagine the kidney cancer as an orange, if there is a positive margin that means there is a piece of the peel that is left behind. For kidney cancer, a positive margin potentially means there is an increased chance of the cancer coming back.
Now that the urologist has the mass removed, he/she should also be able to tell you the stage (or level) of cancer as well as your prognosis. This means, what is the chance that you will be living at 3 or 5 years. Now why only that far? Because that is how far most studies will give data for survival on.
10. How are we going to monitor the kidney cancer going forward?
There are two things the urologist will do to follow you in the office. One thing will be to check your kidney function. This will be done via blood work and may just be performed with your primary care provider.
Additionally, the urologist will order imaging, likely a CT or MRI.
The frequency of how often this needs to be performed will be determined by your stage and what treatment was done. For the first couple years, we like to keep a close eye on things to make sure nothing pops up so usually that will mean a CT/MRI every 3-6 months depending on how aggressive the cancer is. As time goes on, then the frequency of how often we need to do surveillance imaging can be pushed out.
The American Urologic Association has guidelines which review the protocols for monitoring kidney cancer. I would ask them if they are following the guidelines recommendations when determining how frequent to do your x-rays.
In general:
- CT or MRI at 3-12 months following surgery
- Then based on the stage, you will need CT or MRI every 6-12 months for the first several years